
Background statement
Improving health in developing countries require an interdisciplinary approach to sustainable development. Apart from the healthcare delivery itself, several factors put millions of people's health at risk (hazardous water contaminants, lack of education, out-of-date drugs or facilities). Any improvement attempt should include simultaneous interventions in order to create effective, long-lasting results.
Infrastructures
Shortage of qualified health workers and supplies, equipment, and drugs limits ability of health facilities to provide effective services. Depending on the country, the network of infrastructure in Sub-Saharan Africa includes health posts, dispensaries, and/or rural maternities. This first level of healthcare system plays the role of interface between the population and the higher-level facilities like district and other hospitals.
These structures served about 80% of the population but regrettably receive at best only 20% of the financial resources. Hospitals are mostly located in the urban area as where only 30% of the population lives. And even if the hospitals receive most of the health budget, it is found to be dilapidated, there is a lack of medical equipment and other essential supplies. Limited funding and inadequate logistics in association with poor and inequitable access to basic social services like water, sanitation and housing, and high population growth rates, have aggravated the vicious circle of poverty and created a dissolution of the family, social and community identity.
Healthcare Delivery
Human Resources
 Most countries in sub-Saharan Africa are currently facing an array of healthcare finance and management. The region lacks qualified health workers and countries have to train community health workers and village health workers to promote the delivery of basic, cost effective services to the majority of the people. The main problem is that about half of the medical graduates move within a few years after graduation and some of the reasons for this are poor working conditions, lack of opportunities for professional development and clear carrier path, conflicts or wars, and search for better salaries. Migration of skilled health workers have contributed significantly to deteriorating access and quality of care in Africa, reducing the capacity of health systems to deliver health care to the local populations.
Most countries in sub-Saharan Africa are currently facing an array of healthcare finance and management. The region lacks qualified health workers and countries have to train community health workers and village health workers to promote the delivery of basic, cost effective services to the majority of the people. The main problem is that about half of the medical graduates move within a few years after graduation and some of the reasons for this are poor working conditions, lack of opportunities for professional development and clear carrier path, conflicts or wars, and search for better salaries. Migration of skilled health workers have contributed significantly to deteriorating access and quality of care in Africa, reducing the capacity of health systems to deliver health care to the local populations.
Integration within the community
A number of health programs utilize community resources persons, such as community drug distributors, community health workers, and traditional birth attendants among others, in an attempt to coordinate health efforts between traditional, spiritual and westerners health workers. The possibility of building on such a long tradition of community organization is a great opportunity in addressing health issues and strengthening the links with community structures and members. There is a need for a more coordinated approach, to promote more inter-sectored collaboration and cooperation with the different health stakeholders, reform health sciences education integrating skills in planning, financial and personal management. Community involvement needs to be strengthened and resources allocated better. Without an overall approach including all communities and areas, the hope for long-lasting improvement in health care in sub-Saharan Africa is weak.
Lack of coordination
 The successive crisis of the 80s and 90s aggravated the capacities and limitations of the public sector to respond to the needs of the population. Despite the fact that some countries have adopted an integrated approach and initiated coordination within the ministries to address healthcare problems, the lack of coordination among different health providers such as donors, NGOs, private sector and the communities remains evidence. To avoid duplication of efforts, a synchronized approach between departments such as health, environment, labor, and agriculture is needed. In addition, for successful results people need to be involved at grassroots levels and managers of lower structures in the healthcare hierarchy.
The successive crisis of the 80s and 90s aggravated the capacities and limitations of the public sector to respond to the needs of the population. Despite the fact that some countries have adopted an integrated approach and initiated coordination within the ministries to address healthcare problems, the lack of coordination among different health providers such as donors, NGOs, private sector and the communities remains evidence. To avoid duplication of efforts, a synchronized approach between departments such as health, environment, labor, and agriculture is needed. In addition, for successful results people need to be involved at grassroots levels and managers of lower structures in the healthcare hierarchy.
Financial aspect
Financial resources have not expanded to cope with the increasing demand for health care. The poor health investments are mirrored in the life expectancy and the maternal mortality rates. The latest is the highest in the world, mostly due to a lack of access to reproductive health services and a quasi absence of hygiene structures in health facilities located in rural areas. The average life expectancy in sub-Saharan Africa is only 48.7 years, but the numbers vary significantly among countries. Furthermore, about 215 million people in sub-Saharan Africa suffer from chronic under-nutrition.
Diseases and supply
The predominance of AIDS and malaria creates such an important need for health care that health facilities are filled more and more with AIDS related cases than any other cases, at the expense of the other common ailments. AIDS consumes the larger portion of the meager budgets of health facilities and has led to burnout of the health personal that attend to these cases. This also means that fewer and fewer resources are available for essential medicines and supplies.
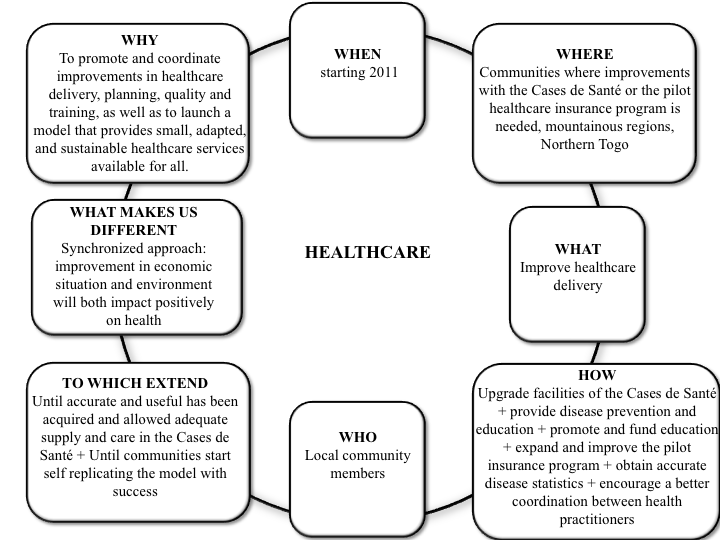
Where we intervene
 Smallest West-African country, Togo faces a high rate of poverty (62% of the population), a longlasting economical and sociopolitical crisis, and a suspension of the international aid. Only 26% of the population has access to sanitation, 12% to electricity and the life expectancy is only 55 years. According to the government in 2006, almost seven of every 100 babies died in childbirth, 49 % of births were unattended and there was less than one doctor per 10,000 residents - the minimum recommended by World Health Organization to guarantee basic health service. Average medical spending is 22 USD, 34 being the minimum recommended by said organization. This being average statistics for the country and knowing that solely 36% of the Togolese population lives in urban areas; the Foundation has decided to intervene in the Northern region of Les Plateaux, around La Kara, in order to upgrade the existing health system in rural communities. The International Foundation for Global Health and Development strives to emphasize and synchronize improvements in health care delivery and make small, adapted, and sustainable healthcare services available for all. We seek an overall amelioration focusing on primary needs, providing disease prevention and education, upgrading the system of the Casas de Sante, encouraging a better coordination of the existing system and promoting self-funding health insurance within the community.
Smallest West-African country, Togo faces a high rate of poverty (62% of the population), a longlasting economical and sociopolitical crisis, and a suspension of the international aid. Only 26% of the population has access to sanitation, 12% to electricity and the life expectancy is only 55 years. According to the government in 2006, almost seven of every 100 babies died in childbirth, 49 % of births were unattended and there was less than one doctor per 10,000 residents - the minimum recommended by World Health Organization to guarantee basic health service. Average medical spending is 22 USD, 34 being the minimum recommended by said organization. This being average statistics for the country and knowing that solely 36% of the Togolese population lives in urban areas; the Foundation has decided to intervene in the Northern region of Les Plateaux, around La Kara, in order to upgrade the existing health system in rural communities. The International Foundation for Global Health and Development strives to emphasize and synchronize improvements in health care delivery and make small, adapted, and sustainable healthcare services available for all. We seek an overall amelioration focusing on primary needs, providing disease prevention and education, upgrading the system of the Casas de Sante, encouraging a better coordination of the existing system and promoting self-funding health insurance within the community.
Vision
To promote and coordinate improvements in health care delivery, planning, quality and training, as well as to launch a model that provides small, adapted, and sustainable healthcare services available for all.
- The Foundation's vision is to significantly but locally improve healthcare in rural communitites by setting in motion progressive changes in the following areas:
- overall amelioration focusing on primary needs
- Providing disease prevention and education
- Encouraging a better coordination of the existing system and coordination in care between healers
- Promoting self-funding health insurance within the community
- Ensuring availability of financial resources, medical tmaterial and treatments
Improving Healthcare
In sub-Saharan Africa, healthcare delivery systems are grossly inadequate. Diseases such as Malaria, Tuberculosis, and HIV/AIDS result in significant death, illness, and compromise of productivity.
In Togo, there are:
- One hospital/clinic for every 8500 inhabitants
- One doctor for every 12,470 inhabitants
- One midwife for every 9,330 inhabitants
- One nurse for every 3,093 inhabitants
- According to the WHO, every 30 seconds a child dies of malaria. The African Region is the most effected by malaria and accounts for about 86% of the estimated 247 million cases of malaria worldwide in 2006 and 91 % of the malaria deaths in the same year. In Togo, 25 % of all deaths of children under five are malaria related and 791,000 malaria-death related cases were reported in 2001.
The number of estimated deaths in Togo dues to tuberculosis is 9,058 in 2007, and the tuberculosis death rate is 138/100,000 population. The tuberculosis incidence per 100,000 population has been increasing steadily over the past 20 years, raising alarming concerns among the population and health entities over the world.
The incidence of Tuberculosis is per 100,000 population:
Year / Value
1990 / 307.6
2000 / 374.2
2007 / 429.2
HIV/AIDS is spreading at an alarming rate in Togo: 130,000 Togolese live with HIV/AIDS, and the number of estimated death due to AIDS as of 2007 is 9,100. In Togo, only 1 in 10 adolescents has a thorough understanding of HIV/AIDS and the ways it can be transmitted, as a consequence, HIV/AIDS is highest among men age 20-30, and women 15-19.
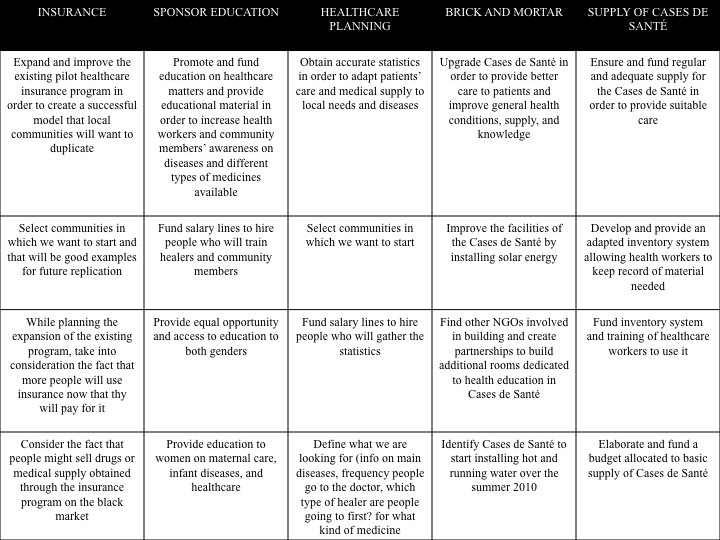
- Modernization of existing healthcare facilities: Brick and mortar projects include: building showers, roof renovation, installation of solar panels for electricity, insulation, and the provision of hot and cold running water.
- Collection of disease incidence data and healthcare statistics to help predict resource utilization and future funding needs.
- Support of local health care system with basic needs:
 Providing medicines, bandages, antibiotics, diagnostic tools, and medical equipment (including stethoscopes and blood pressure tests)
Providing medicines, bandages, antibiotics, diagnostic tools, and medical equipment (including stethoscopes and blood pressure tests)
- Continuous support of the healthcare insurance program:
- The foundation has already developed and funded a basic healthcare insurance program where healthcare services and discount medication are offered for $3.50 per family per year.
- Education: Sponsoring and support of local continuing medication education seminars for local practitioners in order to improve patient care and insure uniform healthcare delivery.
- Epidemiological modeling in order to help predict, detect, and prevent epidemic.
Coordination of efforts between traditional herbal healers, spiritual healers and western style healthcare providers for complete healthcare coverage
These efforts have been successful at multiple levels. All healthcare providers are educated as to the nature and definition of acute and serious disease. This has resulted in agreement to refer the most serious illness directly to the modern medicine clinics for timely treatment.
Non-western style medicine healers are being taught to diagnose and recognize disease such as malaria, hypertension, infectious diarrheal disease and Tuberculosis, in order to obtain more a complete picture of disease incidence and timely care. This will also speed recognition and control of epidemics
Trust among all providers is reinforced and quality of patient care is improved.
Successful non-western style treatments for disease can be recognized, analyzed, utilized, and catalogued for future learning.